
Health care delivery is worth a policy debate; but Senate bill is not that
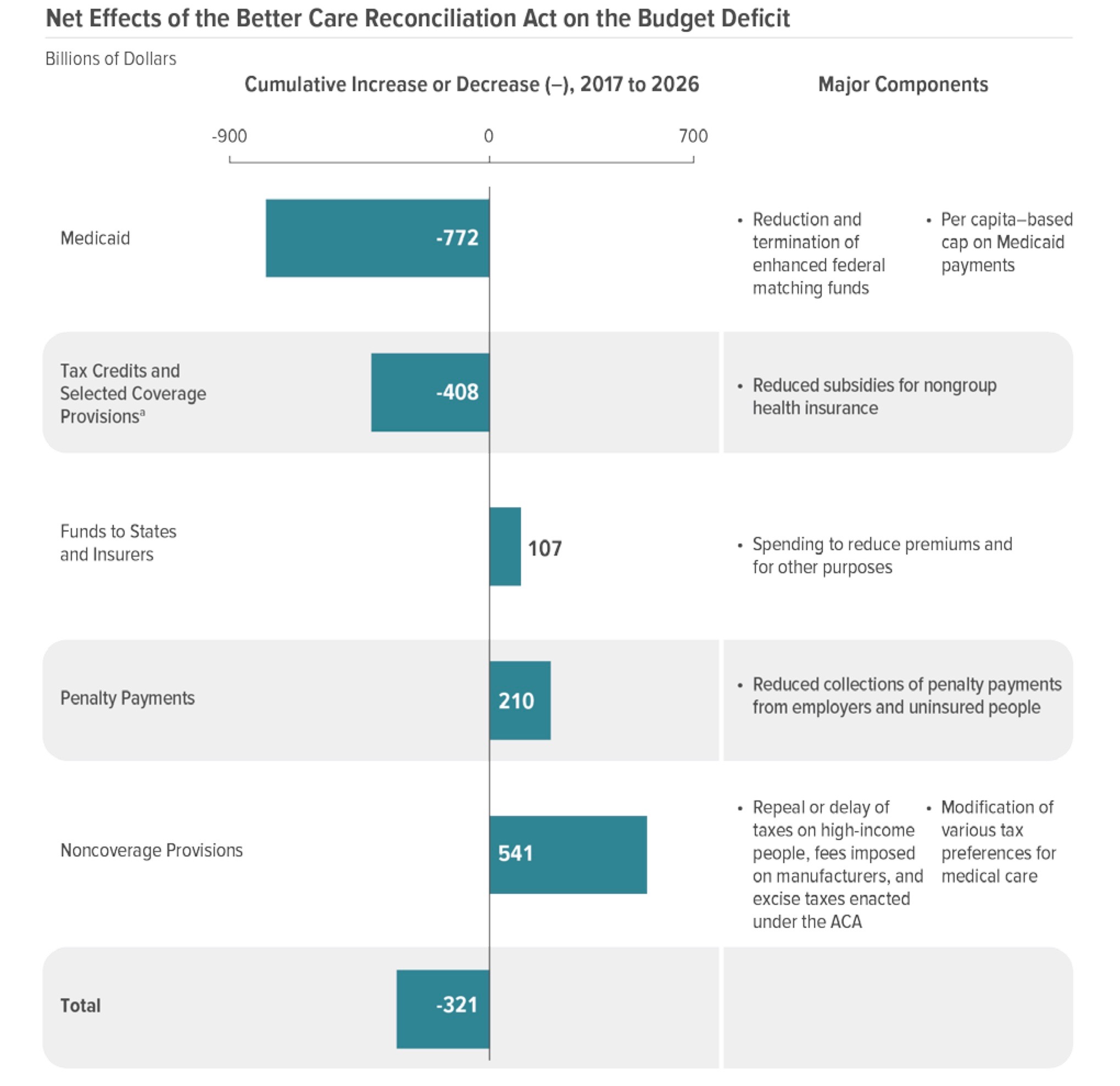
By Mark TrahantTrahantReports.Com The Congressional Budget Office report on the Senate majority’s health care bill — the ironically titled “Better Care Reconciliation Act of 2017” — ought to be enough to put to rest any idea that Republicans want to improve health care in this country. There are legitimate conservative ideas about how to reform health care. You know, the stuff they have been saying for years about market-based reforms where people can shop for their doctors and clinics online across state lines. Think Amazon. Modern, high tech, affordable care. But that’s not on the table. Instead the House and the Senate are trying to legislate a huge tax cut, make a small dent in the long-term federal spending, trim spending on insurance subsidies, and the destroy Medicaid (and, as a bonus, shift responsibility from Washington, D.C., to state governments.) Here are the numbers to back up that paragraph: CBO says the tax cut is worth $541 billion. The long term deficit reduction totals $321 billion. Getting rid of insurance subsidies under the Affordable Care Act saves $408 billion. And recasting Medicaid as a block grant (as well as phasing out the expansion) is worth $772 billion.
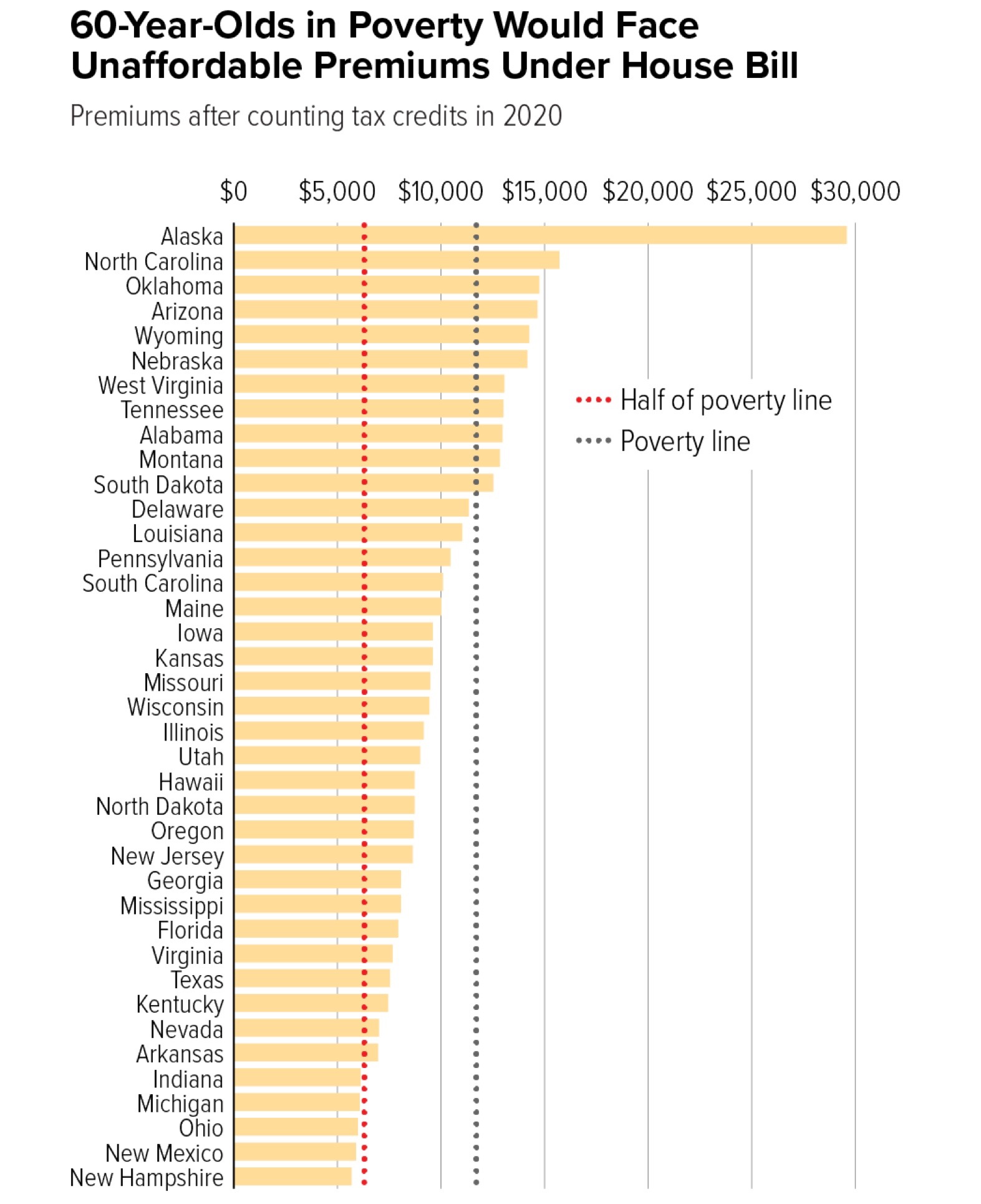
Neither the Senate nor the House bill accomplish any health care goal. Neither bill will help people get insured. CBO says “in 2018, 15 million more people would be uninsured under this legislation than under current law—primarily because the penalty for not having insurance would be eliminated. The increase in the number of uninsured people relative to the number projected under current law would reach 19 million in 2020 and 22 million in 2026.” And down the road when Medicaid reflects “lower spending” that too would “lead to increases in the number of people without health insurance. By 2026, among people under age 65, enrollment in Medicaid would fall by about 16 percent and an estimated 49 million people would be uninsured, compared with 28 million who would lack insurance that year under current law.” CBO says that even employer-based health care would shrink. The crazy thing is that older people would be impacted the most by both the Senate and House approach. As the Center for Budget and Policy Priorities reports: “For people age 60 or older with income at or below the poverty line, individual-market premiums would consume at least 45 percent of their income. The share would be even higher in higher-cost states and for people at lower incomes.” And that’s where geography impacts Indian Country. Alaska, for example, would have the highest cost in the nation. In fact: If you are 60 and trying to buy insurance … it’s basically unaffordable. Insurance costs will far exceed affordability in North Carolina, Oklahoma, Arizona, and Wyoming. This is what’s so important to the Indian health system. Instead of getting funding from third-party billing — mostly Medicaid — the Indian Health Service would have to rely almost entirely on appropriations. The bottom line: There will not be enough money. Remember both the House and the Senate want to convert Medicaid to a block grant. This is not just rolling back Obamacare, it’s returning health care to before Lyndon B. Johnson’s Great Society programs. As the CBO puts it that will lower Medicaid participation by 9 million in 2020 and by more than 14 million by 2026. That’s a lot of people.
Most of the discourse about Medicaid centers on health care. But the program also provides long-term care to elders and disabled in assisted care or in-home care. The way this program works: You give up your assets (except Trust-based assets) and then government promised to pay for your care. The Centers for Medicare and Medicaid say American Indian and Alaska Natives are a fast growing population that already rely on these services. “Between 2000 and 2010, the number of AI/AN adults 65 years or older increased by 40.5%, a growth rate that is 2.7 times greater than that of the overall population of older adults (all races) over the same 10-year period. The AI/AN elder population is projected to reach 1,395,000 by the year 2050; that’s a 3.5-fold increase from 2010 to 2050. In addition to studies that reflect the growing population of older AI/AN adults, other studies have revealed that AI/ANs suffer a disproportionately higher rate of disabilities including (lower body) functional disabilities that increase this population’s risk for falls, demonstrating a clear need for LTSS within this population.” So if the Senate or House bill becomes law future services — as the need grows — will be sharply curtailed. And I can’t answer what will happen to people living in nursing homes now. If a state cuts the payment to a private facility, they could, in theory at least, ask people to leave. Let that sink in. People who have given up everything to live in an extended care facility could end up with no place to go. It will all depend on state legislatures or tribal budgets. I am used to looking at both sides of any issue. I’m interested in views different than my own and exploring whether they have merit. As I wrote above: There is a conservative approach to health care that’s worthy of debate (I’d likely still come down on the side of single-payer.) But the House and Senate bills are not it. The only ideology at work is a tax cut; a painful tax cut at that. Mark Trahant is the Charles R. Johnson Endowed Professor of Journalism at the University of North Dakota. He is an independent journalist and a member of the Shoshone-Bannock Tribes. To read more of his regular #NativeVote16 updates, follow trahantreports.com On Facebook: TrahantReports On Twitter: @TrahantReports
Join the Conversation